A closer look at age of first exposure to football and later-life cognitive impairment in NFL players

This is in part a response to a thread a couple weeks back where I posted a link to the new study by Robert Stern and Julie Stamm et al in the journal Neurology that shows an apparent causal relationship between age of first exposure (AFE) to football and cognitive impairment in NFL players. The comments to the original thread hit a full spectrum that can be honed by a close reading of the study and past work on CTE. A few things have happened since that post that make this more interesting; the Super Bowl for one, John O’Korn transferring into Michigan for another and a civil lawsuit filed against the national office of Pop Warner football for the wrongful death of Joseph Cernach. I’m going to take a closer look at the actual data from the new study to refute some points made in the previous thread (including my own). Then, I’m going to apply this new data to previous studies and finally I will present my opinion as to where these and other recent events are leading.
First the latest CTE news story in which a suit has been brought in a federal court in Wisconsin against The Pop Warner Foundation stating that Pop Warner failed: to train coaches, to use safe helmets, to limit contact in practice, to teach players to use safety equipment and finally, failed to follow established concussion protocols dating back to 1997. The suit was filed by Debra Pyka, mother to Joseph Chernach who suffered from CTE having been diagnosed after he committed suicide at the age of 25 in June of 2012. Joseph played Pop Warner from the age of 11 in 1997 to 14 in 2000.


This is Joseph (a Michigan fan) with mom on the left and Joseph in happier times on the right. Photos are taken from Joseph's donor page at the Sports Legacy Institute (SLI) website and from photos supplied by the family to news outlets.
Fixed tissues from Joseph were examined by Ann McKee at the Boston University Center for the study of Traumatic Encephalopathy (CSTE.) His case was classified as stage 2 - possibly stage 3 and remarked as one of the worst for his age. Joseph’s complete brain was evidently not sent, preventing definitive staging.
This wasn’t the only suit filed in the last weeks but it got my attention and brought back the issues put forth by the CSTE study that came out on Jan 28th. It is important to grasp what that study is saying if only because we are likely to get many more lawsuits like the one above in the near term as well as a continued flight from youth football (participation already being down 29% since 2008.) But these are not the only reasons.
The study in question is entitled
Age of first exposure to football and later-life cognitive impairment in former NFL players
If you haven’t read it and are able to do so… just do it. It’s not that technical. Pundits in the media, however, and others continue to misconstrue its conclusions and validity which is another reason for this diary. What follows here is my understanding of the data presented with sincerity if not authority. It’s clear from the comments to the original board post that many were interested in the work but didn’t have the time to research the journal article.
The study is a cross sectional analysis for causal factors to explain actual cognitive impairment found in a sample of NFL players. The researchers pulled only from those players who were known already to exhibit cognitive, behavioral or mood symptoms in the 6 month period prior to participating. That is what a cross-sectional study is – a cross section of a population. There is no control group. A control is not needed for this sort of examination.
The subjects were pulled from a group of about 150 players who were vetted so as not to have any previous central nervous system (CNS)disorders (no Parkinson's, Alzheimer's, epilepsy or any other incoming disorder.) That cuts out quite a few.
The remaining subjects were then paired by similar age and different AFE to FB (one <12 the other >=12.) Current 10 year old (y.o.) FB players get different coaching and different equipment than 50 y.o. ex-FB players did 40 years ago. This pairing controls for the era of football – as the game has evolved year to year since it was first played but specifically in the living history of the NFL players in the study. The older players did not have as much opportunity to play youth football which further limited the possible pairs.
After all the selection is done only 42 players remained in the study population, 21 in each AFE group. There has been much talk about what exactly you can determine from a sample size of only 42 players. Well it turns out you can do quite a bit. Below is the breakdown of the demographics in the study taken from the article.
")
Looking over the demographics AFE to FB is the primary discriminate along with lesser but significant difference in duration of play(DOP). The confounding nature of DOP and AFE is a valid caveat to any conclusion drawn from this cross section of subjects. Maybe instead of the AFE it is the total number of hits taken that determines later life cognitive impairment. DOP (and age – which is not confounded due to the paired experiment design) was however accounted for and adjusted for in the analysis to focus on AFE.
Three tests were chosen for the analysis (given their focus on the theoretical cognitive deficits expected in CTE) and these were summarized in 9 scores. These are below in unadjusted and adjusted form in the exact data tables published in the journal Neurology.


All the tests are significantly lower for the AFE <12 group. While any significance is interesting, all of the measured outcomes being significant and lower is even more so. Yes, there are only 21 players in each group, but the significance of each of these scores is very high. Suppose you flipped a coin nine times and it came up heads all nine times… you would look at the other side of the coin wouldn’t you? Suppose it came up heads 189 times. That is all this preliminary study is saying. Youth football is a factor in the type of cognitive impairment associated with CTE in NFL players.
In retrospect this confirms a previous study on CTE in December of 2012 done by Ann McKee and Robert Cantu et al though the age of first exposure to the repetitive head injury was not suggested there. Let me suggest that now. That study was appropriately entitled
The spectrum of disease in chronic traumatic encephalopathy
The study included 85 recently deceased subjects known to have suffered repetitive mild traumatic brain injury (mTBI) along with a control group of 17 subjects with no history of the mTBI. The brains of these subjects were donated to the study for neuropathological evaluation along with an independent and blind parallel series of post mortem interviews with next of kin to determine case history.
68 of the 85 subjects showed signs of CTE(80%), while 51 of the 85 subjects were diagnosed with CTE exclusively(60%.)
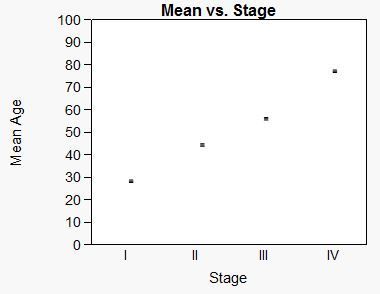
From the pathology a staging system is laid out to which the behavior and historical data are spliced. Part of this historical data is the age at time of death. I took the liberty to put that into an excel table below.

Here is the same data graphically represented next to the iconic images of the staging done by Ann McKee in this study.

What hadn’t occurred to me (and isn’t done in McKee’s analysis either for that matter) was to take this age at time of death data and extrapolate back to stage 0 which given the progressive model for the disease would be the time the CTE started.
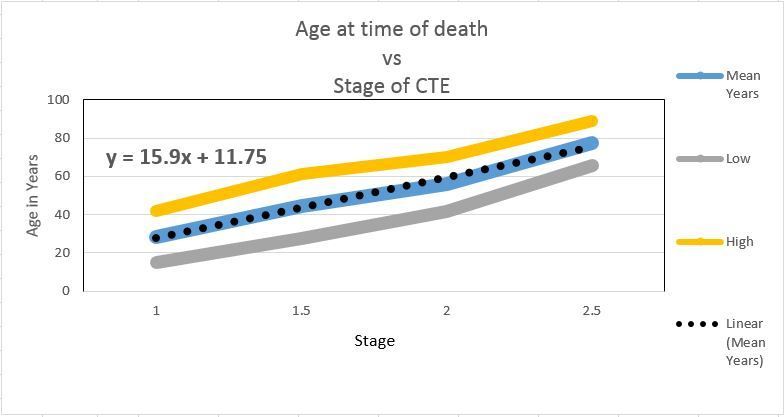
Here’s the same data with a linear regression.

Admittedly this is an N of 51 and only 33 of these are NFL players. The implication, however, is that CTE started at age 11 and 3/4 years old on average. This is a possible reason for the new study in the first place.
All the studies are calling out for more longitudinal designs to be funded and carried out. That would be about right if two sorts of people were doing the calling out. One would be the scientific sort who are careful with their claims and mindful of their funding. The other sort would be the watchdogs of the sport. That would be the NFL executives and owners.
For the rest of us these cross sectional studies will do just fine. There is no way I would ever ever let my son play the game of football as long as he was a minor in my charge. You don’t need broad based studies to find cause. It wouldn’t take too much convincing if he showed resistance.
There is obviously much more to these studies than I’m relating here. I encourage you to look for yourself to ferret out the details you might be interested in.
Cherry picking studies and data from science journals is a good way to get off base and picked off on a college football blog. I do want to present this table however, again from McKee and Cantu’s spectrum snapshot in 2012.

This is tying together the case histories (gathered by Robert Stern who is another author of the Spectrum paper.) From this chart you can begin to get a clinical take on what the progression of this disease is like. I’m showing this because there were some people who responded with either denial, disdain or ignorance to the dangers here.
This is from the FAQ at BU CSTE
The symptoms of CTE include memory loss, confusion, impaired judgment, impulse control problems, aggression, depression, anxiety, suicidality, parkinsonism, and, eventually, progressive dementia. These symptoms often begin years or even decades after the last brain trauma or end of active athletic involvement.
Roger Goodell in the many interviews from Super Bowl week was happy to point out that hits to defenseless players are down 68% in 2014 (yes they track that), concussions were down 25% and that concussions in the past three years have dropped from 173 a season to 111. I doubt they track or could track the sub-concussive blows that are likely the true culprit in CTE.
Still we got the Edelman hit with 11 minutes to play in the 4th with no concussion protocol or independent review during or after the game. It’s going to be impossible to take the football out of football no matter how much you deflate it.
This has already gone too long. I’ll save you my thoughts on where we’re going from here. But I do think Harbaugh took O’Korn and Oregon took Adams for reasons that aren’t entirely unrelated. You can’t have enough QBs in the games to come.
Go Blue!
February 16th, 2015 at 10:11 AM ^
In evidence-based medicine they have a rule of thumb about when a study design is definitive, often called the evidence-based pyramid. A cross-sectional sample of a self-selected population is above "no data at all, it's just doctor's guessing," but is otherwise at the bottom of the pyramid. Cross-sectional evidence means you can't assess causality. More concerning, the brain samples they used were people who contacted them. There is no way to know that there wasn't any of a million reasons about who showed up to donate causing the results. You say "A control is not needed for this sort of examination." This is true, but only because this is a scientifically relatively poor sort of examination.
Actually, they did use a control group, even though they said the didn't. It was self-reported AFE>=12. All their statistical analyses are done comparing the AFE<12 to them. That's a control group. That said, the control group is a problem. Ideally they would be identical to the "intervention" group (AFE < 12), except for the intervention. That's unlikely to be true here, since the samples were all self-offered, as opposed to being randomly from all NFL retirees, or something more consistent. Notice, BTW, that the two studies are overlapping research groups at BU and the nearby VA.
That's not to say this is bad science or that it's wrong. If I were peer-reviewing these papers (I'm not a neurologist, but I do review somewhat similar stuff in my field) I would probably accept them both, mostly because the potential of this field is so important. It is very preliminary work, though. It has many possible ways that the results could be false-positives.
What's that say about parenting? Judgment call. This is concerning. Football certainly isn't good for the rest of your body and it's easy to imagine this being accurate. I'm worried.
February 16th, 2015 at 10:39 AM ^
parsing the word control here. A true control would have been a group in the same age group that had not played football or any other contact sport. But then the study clearly is relative to their hypothesis that the age of first exposure correlates to greater cognitive impairment in later life specifically using the age of 12 to define the 2 groups and therefore does provide the control. It would be interesting to see the study expanded to include those playing between 12-18 compared to a true control group. I liked the previous study as well that used pathology examinations to make this determination.
This study confirms what we all know is true intuitively and as much as we love football, allowing kids prior to the age of 12 to play a contact sport like football is a very poor idea.
February 16th, 2015 at 11:35 AM ^
I don't want to be pedantic, but what you're describing as a control is a control to answer a different question. Their question is "is tarting football before age 12 is associated with higher rates of CTE?" Yours is "Is playing football or any other contact sport associated with higher rates of CTE?" They're both legitimate, but they're asking the first one. It happens that the question in this paper is not the single most important one in this field (which is the one you asked), but it is a wothwhile study with a not-crazy control for a reasonable hypothesis. They then assess that in multiple ways, using siginficance testing to compare their intervention group to their control. That's what table 3, in particular, is all about. They and their peer reviewers should have made sure it was written that way. Again, this is hardly the greatest sin possible in a study.
February 16th, 2015 at 12:19 PM ^
we are sort of saying the same thing actually-its relative to the hypothesis. The flaw in their approach was that they could have found no difference between the 2 groups and that it wasnt age related, however compared to a nonfootball population there would be a difference. They likely had some data to support their stated hypothesis that it was age related and therefore kind of got away with this hypothesis. If this was a grant proposal they would have had to include a non football population to cover this likelihood.
The greater question really is what will the football powers that be do about the overwhelming evidence now emerging that concussions lead to significant disability later in life? My guess is there will be guidelines for those under 12 eventually. Really how do you ameliorate concussion risk when two people run at full speed toward each other and collide? You can't unless you change the game to touch football.
February 16th, 2015 at 6:49 PM ^
You mean like every single sport offered to kids? Is it intuitive that kids should not play soccer, basketball, baseball, or even climb on monkey-bars? I've coached youth sports in all of those sports across three children, and the contact in other sports is just as significant as football. In fact, that is one of the first things I tell my teams while coaching soccer and basketball.
Kids bang heads running full speed at each other all the time in soccer. Kids fall and hit the back of their head in basketball often (happened to one of my boys last weekend). How about an errant pitch to the helmet in baseball - those 10 yr old pitchers don't have much accuracy yet. These would all be of the sub-concussive variety the OP says are most dangerous.
So what should we do, pull everyone off the fields until they're 12? Seriously.
February 17th, 2015 at 12:21 PM ^
Just my feelings on this so take it or leave it....
I have an 10 year old boy who will be going into his 4th year of tackle football. I watch the games and practices as closely as I can and, for now, I've decided that what I see doesn't look too risky and the benefits of playing outweigh the risks. Also, there is far less helmet to helmet and unnecessary contact than there was when I played at that age. I loved my little league coaches and certainly hold no animosity against them, but it was the 70s/80s ... we'd grab each others' masks and pull our helmets together as hard as we could, played a psycho game called bull-in-the-ring, lots of shit they don't do today.
All that said, you can't call out football as being equivalent to basketball or baseball. The number of impacts aren't even in the same order of magnitude. If football's impacts to kids are going to be addressed, we need to be honest about it.
February 18th, 2015 at 9:55 AM ^
February 18th, 2015 at 10:06 AM ^
The impacts sustained by childred from heading the ball may be very damaging. This surprised me when I heard it, but apparenty it's a big deal.
I always cosidered hockey just as dangerous as football when it came to head injury, but I suspect you're absolutely right. Watching those little guys trying to line each other up is hilarious. Alternatively, the violence of high school hockey is surprising. Those kids do skate well enough to be dangerous and really want to hurt one another.
February 17th, 2015 at 10:19 AM ^
Does it prove cause. No. Does it find cause. Yes.
If cross sectional study is "poor" by definition then I can't argue that point. There is a good reason this study was done as it was given the resources and money we have now.
Note Stamm used established neuropsychological tests that can be compared to larger population norms. All subjects were below average in this respect.
Unfortunately the issue of mTBI is not restricted to football. If it were, we might never get a "rich" study done. The military has great need to actually determine the effect of long term mTBI. That will certainly provide answers in the long run. As a parent, I can't wait for that.
I also work in a technical field where design of experiment is paramount. Public health doesn't operate in that zone. Case controled studies are not initailly or ever possible for ethical, monetary, social or practical reasons.
What is your judgment sj? When kids can play team sports that don't involve contact like that dictated in tackle football (like Ultimate or Flag Football) does your son don the helmet or not? Troy Aikman and Terry Bradshaw say no. They don't need studies period. What do you say?
February 17th, 2015 at 12:01 PM ^
Thanks for the great thread!
If you had to guess, what is the cause for the effect of age differences? What happens to around the age of 12 that makes a difference?
If soccer players are also exhibiting CTE, it would be interesting to do a similar study and see if you get a gender difference in the cutoff age (e.g., boys - 12, girls - 10).
February 17th, 2015 at 4:03 PM ^
of the study. I can paste data but not discussion due to copyright (I'm pretty sure that is right - better to be safe than sorry.) Stamm suggests several models for this. Personally I have no idea but I'm reading about this myself at the moment trying to understand.
I'm also very interested in the progression of the disease. I'm not sure how that works either. Any clues on that from readers would be appreciated.
February 17th, 2015 at 5:57 PM ^
Thanks. I'm not a neurologist, so I don't understand how concussions could lead to potential loss in mylination. Definitely a fascinating topic and hopeully we'll learn more as research on this topic ramps up
February 16th, 2015 at 12:40 PM ^
it was flag football with gear and no tackle until high school and this was 40 years ago . I do not remember how aggressive the blocking was so the contact may still have been there but it seems that the school was trying to limit contact. Are there areas of the country where schools allow full contact prior to high school ?
February 16th, 2015 at 12:55 PM ^
Sent from MGoBlog HD for iPhone & iPad
February 19th, 2015 at 9:19 PM ^
February 16th, 2015 at 1:45 PM ^
Ann Arbor native here. I started playing organized football when I was in 5th grade (to age myself, that was about 20 years ago). Fun fact, Eddie Brown (MSU db who tripped Desmond in the endzone) was one of my coaches and was very open about the fact he tripped him on purpose. Anyways, in case it's specific to your question, this was not a school team as I don't believe any Michigan public Middle or elementary schools do football teams.
It was full contact tackle, and really the only limitations was that there was 3 different tiers from like 4th/5th graders to 8th graders, with a specific weight limits in each group. Weigh-ins were before each game and if you were so much as a pound over the limit, you tried to run it off quickly before the game (ala wrestling style) or you sat on the sidelines. This meant you would certainly get hit and hit hard, but only by kids around your same age and weight. And yes, during even back then, not leading with your helmet or going after someone else's was preached ad nauseum.
So to answer your question, full contact football certainly was still a thing as of the mid to late 90's. Last I heard, the team I was a part of later became the Ann Arbor Junior Wolverines, which is still active I believe. Though I don't know for certain if it's still full contact, I believe it is. I'd have to imagine much less kids are on the teams these days, and I know if I had a son, I wouldn't let him play.
February 18th, 2015 at 10:36 AM ^
I played QB on the Jr Wolverines in the 70s opposite one Jr. Packer team that in my 12th year did not even make the championship which we won. Glory days.
February 21st, 2015 at 7:25 PM ^
Yep... my kid plays for the Maize squad.
February 16th, 2015 at 1:46 PM ^
1). If this is what happens how do you cushion your brain from the skull?
I feel helmets do a pour job of protecting your brain (I know shocking), but they do a good job of protecting your head to other injuries, and this feeling of protection causes players to use it as a weapon. So is there a way, kind of like cars with crumple zones, to slow your head down so your brain doesn't hit your skull so hard?
2). Are there certain parts of your brain that are more susceptible to being concussed?
I thought I read somewhere on this blog that a lot of concussions happen when a player hits his head on the ground while being tackled. This makes sense to me because the ground doesn't give and it stops your head, while if you hit something head on your neck provides some form of shock absorption.
3). What kind of force is needed to cause a concussion?
I have a step son that is going to start playing full contact ball next year and I know the concussion issue won't be solved probably until he is done with football. I wonder if going to a Kevlar type helmet or just some other material than plastic would help cut down the impact the hits have on your brain.
Sent from MGoBlog HD for iPhone & iPad
February 16th, 2015 at 3:33 PM ^
I know that Riddell came out with a new helmet this past year that they said had something akin to a crumple zone on the crown of the helmet. I think it was rolled out to a few select college teams as well as in the NFL.
I'm also skeptical of how effictive it will be if a blow to the head does not happen in that "crumple zone," or in a way that the zone was not designed for. I.e. a shearing blow that can be just as harmful to your brain as a head-to-head collision.
February 17th, 2015 at 3:08 AM ^
the design is to allow the helmet to lessen the "dwell peak" that is to spread out a shock in time and space. First, if your head hits the ground there are areas that get higher shocks ( since you may not hit a flat surface the helmet spreads the local areas of high shock over a larger surface area ) , then if the shock is larger the outer shell delaminates and takes up further shock. Finally if the contact is severe and the shock is not dissapated by the shell and being spread out over a larger area, the inner liner is a dense styrofoam which crushes , taking up more shock. Whatever is left over then is dissapated over the skull.
Football helmets can't have the shell delaminate or it would last only a single play. The shock is spread out over a larger area, but the liner can't crush either or it would also be one and done. The best you can do is to lower the peak transmitted G's by lengthening the time the shock is passed on so it would be 1G for 2ms vs a 2G peak for 1ms. The brain mostly is damaged by the peak shock.in motor vehicle accidents but football is a different animal since there are many repetetive small shocks that add up over many years rather than an accident or two. Still I would think reduction of peak shocks in general is still the goal.
February 18th, 2015 at 2:31 PM ^
We'll likely soon find we've hit the limit on cushion technology with respect to concussions. I think you're right - the object is to lessen the brain's blow to the skull or perhaps to limit compression of brain tissue due to impact. Even if we're talking two inches of cushion material, there's no doubt a limit to what can be devised.
Would be an interesting field to be in.
February 16th, 2015 at 7:13 PM ^
Extrapolation can make sense when you have a numerical measurement that varies over time, but using the stages of disease as quantities seems like a real stretch to me. If you're at mile 1 at 1pm, mile 2 at 2 pm, and mile 3 at 3 pm, sure, you probably started at noon; extrapolation makes sense. Headaches and loss of attention at age 30, depression and short-term memory loss at age 45, executive dysfunction and cognitive impairment at age 60, and dimentia, aggression, and word-finding difficulty at age 75 does not suggest something started at age 11 years 9 months. If the symptoms had been selected differently and broken into more or fewer stages, you'd get a different number from the same patient histories.
That being said, I'm glad this was posted and the more attention the topic gets the better.
February 17th, 2015 at 8:17 AM ^
The case histories and symptoms were gathered blindly and independently from the pathology reports as well. The age at time of death is the only case history data drawn here to perform the extrapolation. Each subject is a snapshot of the stage of CTE at time of death.
Extrapolation can work with categorical measurement with or without variance over time as long as there is an ordinal relationship - in this case born out in the data and captured in the excel table. The staging linearity is real and even responds to the variance.
Is it QED. No it is not. Is it a model that makes sense. Yes it is.
Regardless of model or sense - the uncertainty is huge. All caveats apply.
February 17th, 2015 at 8:32 AM ^
You're right that the symptoms I listed don't detremine the staging, but the characteristics that do aren't any more quantitative. The definitions are here, in the Neurological diagnoses section. It's a qualatative evaluation and the numbers I, II, III, and IV don't have quantitative meanings. They're just classifications. If the characteristics had been divided into more classes, since the ages in the data set cover a fixed range and you always start with Class I, the slope would be higher and the intercept lower. With enough classes, you could probably get a negative intercept.
February 17th, 2015 at 11:10 AM ^
That is what allows this admittedly imprecise but accurate extrapolation. It's a gross reality check that the underlying hypothesis in the first study is in the initial study of the spectrum of CTE demographic.
Yes negative intercept is possible if the relation is not linear. But it isn't ... which is interesting if not significant.
February 17th, 2015 at 11:27 AM ^
I'm not suggesting a non-linear relationship. The intercept could be negative with a linear relationship. If you divided the spectrum of neurofibrillary tangle states into 8 classifications instead of 4, those 8 classes would still be distributed over an age range covering 14 to 89. The slope would be much higher (not quite double), the Class I mean age would drop, and that would be about enough to yield a negative intercept. If there were only 3 classes, the slope would be less, the 1st mean age higher, and the intercept higher. The arbitrary number of classes you select has a dramatic impact on what that intercept would be.
February 18th, 2015 at 2:20 AM ^
0.5, 1, 1.5, 2,2.5, 3, 3.5 and 4. This adds a stage lower than 1 but we could do it however we like. The important thing is to correctly classify each subject to the pathological criteria which in this case would be a transitional stage between the existing non fractional stages. That gives the quantitative matching that you mentioned.
If we assume that the regression remains linear then the 0.5 group comes in ~8 years younger than the stage 1 group on average. Data points would likely fall randomly between the higher and lower stages giving roughly the same line. After all the data is the same whether we cut it 4 ways or into an infinite and continuous numerical score of CTE-ness. Granted there will be more noise with more stages but it will be approximate to the four point line. I don't see how an 8 stage cut of the same data is going to nearly double the slope.
If I had the data itself I could do something else with it. But I only have the mean and confidence interval for the stages defined.
In the mean time, pun intended, you can extrapolate a line from this...
to get a stage zero or extrapolate a heisman from Denard's first 5 games of 2010 for that matter. Extrapolation does not always work. As I have said before the confidence intervals are too wide to put much credibility into this GRC... but it's interesting and instructive.
The x intercept of any of these hypothetical myriad stages and linear models would always be non negative, unless we induce CTE in the womb. More data will tell the story.
Plotting the categorical data vs. time of death is problematic for CTE. Though it's likely Joseph Chernach's death is somewhat CTE related - CTE does not kill in general. Instead it denigrates quality of life for the most part. It is unlikely a pathologist would look for CTE in a teenager to diagnose a 0.5 stage brain. There are half the number of stage I brains compared to the other stages with or without any fractional breakdown. Stage IV subjects are older and bounded by natural death as well as failure to thrive. Waiting for a donor to die is a non random sampling strategy.
UCLA has a patent on a PET scan marker for Tau protien that has already diagnosed Tony Dorsett and other NFL vets with CTE. These are later stages but perhaps they will be able to perform these tests reliably on non symptomatic players and bring a real focus on the extent of CTE - supposedly affecting from 3.5% to as much as 30% of all current NFL players depending on whose projections you use.
February 18th, 2015 at 8:39 AM ^
Number the classes I through VIII and you get roughly double the slope. If there were 3 classes instead of 4, they would be I, II, and III, not 1, 2.5, and 4. When you pick the numerical range of the classes, you're arbitrarily scaling the x-axis. Sure, it doesn't change much if you spread the data from 1 to 4 or 0.5 to 4, but spread it from 1 to 8 and you get a different slope. If there were real world significance to the intercept, it wouldn't change based on how you decide to number your classes, but it does matter.
February 18th, 2015 at 10:28 AM ^
Changing scale doesn't change the relationship between variables. The regression formula will be different but the intercept will approximate the same result.
February 18th, 2015 at 11:11 AM ^
I got it backwards when when I specified which way the intecept goes, but if you don't believe me, try it. Use the same mean age values you used in your chart, but change the four stages from 1,2,3,4 to 1,1.5,2,2.5 and find the intercept.
February 18th, 2015 at 12:01 PM ^
with the new criteria for the new staging regime. 1.5 would probably be very near an interpolation of 1 and 2...
The mean age data comes from the distribution of the stage sample of subjects ...
February 18th, 2015 at 1:59 PM ^
Why would the criteria change if you're still breaking it into 4 groups? Or let me ask it differently. Why should the stages go 1-4? Why not 1-3 or 1-5?
February 18th, 2015 at 2:37 PM ^
Great exchange but I think I just got a concussion trying to understand it.
February 18th, 2015 at 4:01 PM ^
it won't change the scale which is ordinal as determined from the mean ages. The stages are noted in roman numerals which is used often and in this case to designate ordinality. The naming convention of the stages has nothing to do with scale.
Ideally we would have an infinite number of stages with a continuous response in age of subject. Staging in medicine wrt disease has an interesting history. Staging in this paper is very precise and was verified by two other pathologists in the study. If another stage made sense I'm sure they would do it. Note stage IV subjects don't do to well so a stage V is unlikely. On the other side however, given the progressive model a stage 0 isn't unreasonable.
It wil not be until 10PM pacific at the earliest - FYI
February 18th, 2015 at 4:37 PM ^
If you designate a stage V, you have to come up with terms that yield stage V subjects. It's like turning the amplifier up to eleven, it doesn't mean anything in absolute terms (that's the Spinal Tap joke), it's just how many divisions you make to your group (or your amplifier power). It's not that you wouldn't have people in a fifth stage because everyone in stage IV is too sick to make it any further; you'd try to construct the stages so that the sickest group of people are in stage V.
February 19th, 2015 at 8:59 AM ^
Check the equation. Here's the last stage. 15.9*2.5+11.75=51.5. It should be around 77. That's the old fit for the previous stages. The linear fit to the line in this plot is y=31.8x-4.15.
February 19th, 2015 at 9:39 AM ^
The regression is to the ordinal scale. If there were 8 stages the slope would be ~8.
You can't change the data/relationship between the variables. I could graph stages 1, 1.5, 2 and 2.5 but like I said before the mean ages would change - not to mention I don't have that data.
I can extrapolate to stage 0 or stage 5 or interpolate to 1.5 or 3.96748. I can't change the nature of what a stage is (as determined by a team of pathologists) or the mean age of the subjects by stage.
Humans are pattern recognition machines. Correlating ordinal independent variables to reality is discriminant analysis. That is what staging is in this biomedical context.
February 19th, 2015 at 1:52 AM ^
it's about displaying the data we have which is coming from the microscope and in the case of the later stages the naked eye. Marrying the data to the case histories shows that CTE is a progressive disease.
Stage I = Foci of p-tau tangles
Stage II = Multiple discrete foci of p-tau tangles
Stage III=Widespread tangles throughout the brain
Stage IV=Severe p-tau abnormailities throughout the brain (but oddly not so much the visual cortex...that is weird??)
And your suggesting creating a stage V composed of the sickest group of stage IV subjects. Hmm. OK. That would be your 95 y.o. on average with very little working brain. You start to lose people here to CTE and natural causes.
Whatever stages you map out the relationship between the progression of CTE and age of each subject wrt to their pathological stage is not going to be any different regardless of how many stages you stipulate.
February 19th, 2015 at 9:21 AM ^
The stages they picked may makes sense, but they are arbitray, and they are not quantifiable units of measurement, just classes. It could just as easily be Stage I: presence of foci, Stage II:multiple foci, Stage III: presence of clustered tangles, Stage IV: widespread clustered tangles, Stage V: Severe p-tau abnormalities.
February 19th, 2015 at 9:46 AM ^
The criteria for staging is explicit and verified by two other pathologists in the study. But don't depict the criteria as random or arbitrary. It is neither one.
February 19th, 2015 at 10:25 AM ^
Not random. I'm not saying that and never used that word. The classifications were picked to show the disease in progressive stages. But the decision to make it 3 or 4 or 5 or 8 stages is arbitrary, and the numerical value of those stages does not hold meaning. They show an order; they do not represent a quantity. I'm not challenging anything from the study. Just the idea that the extrapolation of the line to find the intercept indicates something.
February 19th, 2015 at 12:06 PM ^
Unfortunately I can't drink beer now, but I will around 9PM tonight pacific...in case you are checking this thread.
February 19th, 2015 at 1:06 PM ^
That sounds good to me. Local place here is clearing out a supply of Founder's Dark Penance for $3.99/4pk. Beer o'clock can't get here soon enough.
February 20th, 2015 at 1:41 AM ^
why is the correlation so high for age at death? The researchers use Spearman's rho for a correlation check. The correlation is greatest of all variables for age at death (.806) with p<.0001. Why so high? Given the small sample size and large confidence intervals that is a very high correlation. If the staging is arbitrary and the x axis is ordinal I would expect a marginal correlation.
CTE is known to be progressive. The linearity of the staging vs. age at death suggests that McKee got the staging right.
Besides the stats though... the criteria, microscopic and macroscopic images pass the sniff test. It's not clear to me that there isn't some quantifiable measure even in the slides.
Even if the staging is arbitrary the correlation is real. if the correlation is real the extrapolation is not unreasonable. Is it a done deal? No. Like I said in the post... these are cross sectional studies that do not prove cause ... but do find causal relationships.
In the second study a major finding is the correlation of age at death and pathological stage.
Staging for CTE based on post mortem is kind of ridiculous wrt other diseases. There is no real therapeutic or prognostic value when there is no treatment (besides possibly an untested method championed by Bernie Kosar) nor in vivo diagnostic test (besides the promising PET scan marker I mentioned earlier.) McKee stages the disease to enable later studies to build and refine the staging criteria for possible interventions.
This and other studies are bedrock templates for contact athletes who no longer play to begin to ask the questions and come to terms with the possibility that they could have CTE.
No the extrapolation does not prove CTE starts at 11.75 years of age. If you do the regression on the high and low CI that would be a margin between 27.5 years old to ... wait for it ... - 4.25 years old. Yes negative. As I said before negative values don't make sense here though. That on average this comes to 11.75 wrt the fist study is interesting however.
Regardless of the x intercept contact athletes are contracting this disease early in their lives... on this at least let us find common ground. CTE doesn't spring up at stage I without some latency. As McKee mentions there are reasons to believe that the progress of the disease is slower in some of the subjects. The early pre stage I phase post the initial trauma may be a completely different kettle of fish with respect to the growth and spread of the disease. As I also said earlier... Denard didn't win the Heisman in 2010 based on his first 5 games... extrapolation = caveat emptor.
February 20th, 2015 at 9:01 AM ^
I don’t know why the correlation is so high between stage and age, but just that point on its own doesn’t point to the AFE. If there’s a first exposure that starts the clock, that would reduce correlation to age at death since people start playing at different ages.
I agree negative intercepts don’t make sense, but that’s why I introduced the possibility, to illustrate that the intercept doesn’t signify anything. The stages are based on characteristics rather than measured quantities. There’s no obvious reason why the time from Stage 1 to 2, or 2 to 3, or 3 to 4 would be about the same, but it happens to be that way. That says nothing about when the disease started. There’s no reason to believe that the time from when you’d say there are multiple foci of tangles to when you’d say the tangles are widespread indicates the time from the start of the disease to the appearance of tangle foci. Those timespans may happen to be the same, but I don’t think it’s valid to assume they are, which is the essence of making that argument based on the linearity of the line.
February 20th, 2015 at 9:08 AM ^
But I agree with everything else. Carrying on about this one quibble paints me in the wrong light, I'm not a critic of your post, I think it's a great thing for MGoBlog.
February 20th, 2015 at 2:15 PM ^
concerns you raise.
I don't worry too much about how I come off on this blog. These types of back and forth refine my thought, broaden my knowledge and push the topic. I appreciate your time, demeanor and the clarity.
MGoBlog allows a dialogue that holds the OP accountable (including Brian i.e. his Brandon take down and follow) and allows the reader to come to terms without a one and done self validating read through which is standard operating procedure with most media. I'm thankful for that.
Comments